Schizophrenia is a severe mental disorder impacting the lives of approximately 51 million people worldwide every year.1 Schizophrenia is defined primarily as a loss of touch with reality, causing a person to be uncertain of what is real and what is occurring only in their mind.1 In addition to affecting a person’s thoughts, feelings, and behaviors, schizophrenia can also impact an individual’s sex life.2 Although there is no known cure for schizophrenia, there are treatments and resources available to reduce or eliminate the symptoms of the disease.
Table of Contents
Symptoms of Schizophrenia
Individuals with schizophrenia typically begin to exhibit symptoms of the disease between the ages of 16 and 30.2 It is rare, but possible, for children under the age of 16 to develop schizophrenia. Teenagers with schizophrenia experience many of the same symptoms as adults do; however, their schizophrenic behaviors are often misattributed to male puberty and female puberty. Symptoms of schizophrenia in teenagers include withdrawal from social activities, reduced academic performance, difficulty sleeping, irritability or depression, and lack of motivation.3 Many of these symptoms are also often associated with experiencing puberty. Although each person may experience schizophrenia differently, there are three general categories of the most common characteristics of schizophrenia: positive, negative, and cognitive symptoms. In order to be diagnosed with schizophrenia, an individual must exhibit two or more classic symptoms of schizophrenia for approximately one month or more.1 Positive Symptoms Positive symptoms are psychotic behaviors including hallucinations, delusions, unusual thought processes, disorganized speech, and distressed physical movement.1 Positive symptoms are the most severe and most noticeable group of symptoms experienced by schizophrenic individuals. Hallucinations Schizophrenic hallucinations can involve all five senses. Typically, people with schizophrenic hallucinations see and hear things that are not there; however, schizophrenic individuals also report feeling, smelling, and tasting things that are not real.1 One of the most common hallucinations is hearing non-existent voices in their head, often directing them to commit acts of violence or self-harm. Delusions People with schizophrenia often exhibit strong feelings of paranoia, constantly fearing that people wish to harm them. Additionally, schizophrenic individuals may feel that they are receiving personal messages from the radio or television.1 Other schizophrenic delusions include believing that there is a fatal illness inside their body even when there is no medical evidence of such.1 People with schizophrenia also commonly believe that they are divine or God-like, possessing supernatural powers and abilities.1 Thought Processes People with schizophrenia may also experience racing thoughts, jumping from one subject to the next with no apparent pattern or organization.1 These thought patterns contribute to disjointed speech patterns and body movements. Schizophrenic individuals may often appear frantic, disorganized, and manic (restless, energized, agitated, and sometimes reckless).3 Negative Symptoms Negative symptoms are deviations from normal and healthy emotions.1 Negative symptoms include reduced expression of emotions, reduced feelings of pleasure and fulfillment, low energy, difficulty beginning and maintaining activities, and reduced speaking.1 Positive symptoms are typically behaviors, whereas negative symptoms represent a person’s feelings and emotions. Cognitive Symptoms Cognitive symptoms refer to symptoms of schizophrenia that impact a person’s cognitive ability or ability to process thoughts, knowledge, and memories.1 People with schizophrenia may experience varying levels of cognitive symptoms, including poor comprehension and decision-making skills, trouble focusing, and difficulty remembering recent information.1
Risk Factors for Schizophrenia
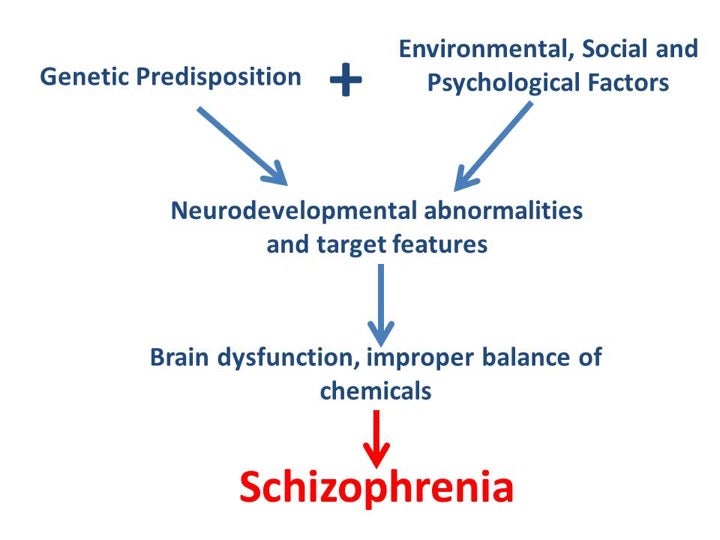
Although the exact cause of schizophrenia is unknown, there are several factors that appear to have a high correlation with the development of schizophrenia. The strongest indicator that an individual is at risk for developing schizophrenia is having a family history of schizophrenia.4 People with first-degree relatives who had a schizophrenia-related personality disorder were more likely to develop schizophrenia themselves than individuals without schizophrenic first-degree relatives. Other risk factors for developing schizophrenia include autoimmune disorders, having an older father, having pregnancy or birth complications, and taking psychoactive drugs during adolescence.3 Schizophrenia cannot be accurately attributed to one specific factor or characteristic; rather, it is more likely that developing schizophrenia results from a combination of genetic predisposition and environmental, social, and psychological factors.
Dangers of Schizophrenia

Individuals with schizophrenia are more likely to engage in violent behavior or suicidal tendencies than the general population.5 Typically, violent or suicidal behavior is a result of a person’s hallucinations or delusions. For example, many people with schizophrenia develop the belief that they can fly or that they cannot be harmed, leading them to test their beliefs by jumping off buildings or other tall structures.5 In other cases, a person’s hallucinations will convince them that their family and friends are going to kill them, causing them to act violently toward their loved ones. Although violent behavior in individuals with schizophrenia is a real possibility, the majority of people with schizophrenia will never endanger themselves or others. Many schizophrenic individuals can develop anxiety or depression surrounding their illness, causing them to feel socially isolated and victimized. These feelings of depression and isolation can prohibit a person from being able to work or attend school, often leading to financial problems or homelessness.3
Sex and Schizophrenia
Most studies show that individuals with schizophrenia do not differ much from the general population in terms of sexual desire. It appears that schizophrenia does not interfere with a person’s overall sex drive.2 Despite similarities in sex drive, it appears that schizophrenic patients experience less intimacy and commitment than their non-schizophrenic counterparts. Lack of intimacy in the sex lives of schizophrenic individuals could be due to a multitude of factors including stigmatization of mental illness, institutionalization, and antipsychotic medications.2 It has also been observed that females with schizophrenia tend to have more favorable sex and love outcomes than males with schizophrenia. Schizophrenic females tend to date, have sex, marry, and have children more frequently than schizophrenic males.2
Schizophrenic Medications and Sexual Side Effects

There is no cure for schizophrenia and most patients require lifelong treatment including medications, therapy, and institutionalization. Medications are the most common form of treatment prescribed to individuals with schizophrenia because they can be effective in reducing schizophrenic hallucinations; however, medications can often negatively impact one’s sexual functioning.
Antipsychotics: Abilify, Latuda, and Saphris are all antipsychotic medications that help treat schizophrenia. Antipsychotics function by altering the effect of neurotransmitters in the brain such as dopamine, noradrenaline, and serotonin.6 Dopamine is the primary neurotransmitter targeted by antipsychotics. Increased levels of dopamine may be responsible for the hallucinations and delusions commonly experienced by schizophrenic patients. The medications listed above have several side effects, including sexual dysfunction. Forty-five to 80% of males and 30-80% of females report experiencing sexual dysfunction after taking antipsychotic medications.7 Antipsychotics are known to decrease libido, interfere with arousal and orgasm, contribute to erectile dysfunction in males, and to decreased lubrication in females.7
Selective Serotonin Reuptake Inhibitors (SSRIs): Individuals with schizophrenia may also develop depression. Fluoxetine, citalopram, and paroxetine are all selective serotonin reuptake inhibitors (SSRIs) which are medications that help treat depression. SSRIs work by blocking serotonin reuptake, increasing the levels of serotonin in the brain. Higher levels of serotonin help to improve a patient’s mood.8 SSRIs can cause most forms of sexual dysfunction, but most commonly patients taking an SSRI experience dysfunctions involving sexual arousal, orgasm, and libido.9 These medications cause sexual dysfunction by inhibiting the production of nitric oxide, which is the main mediator of both the male and female sexual arousal response. Nitric oxide is a neurotransmitter that widens blood vessels to allow more blood flow into the penis and clitoris, the erectile tissues of males and females, respectively. This leads to complaints of vaginal dryness, diminished genital sensation, and often times orgasmic difficulty.9 Potential treatments for SSRI-induced sexual dysfunction include the following:9
- Decreased dosage regimens: Decreasing the daily dosage may resolve or significantly reduce the sexual side effects. If the patient’s complaint is delayed orgasm (i.e. anorgasmia), the patient can be instructed to time intercourse either soon before or soon after taking their SSRI dosage. This timing allows for the drug level to be at its lowest during intercourse, hopefully decreasing sexual side effects.
- Drug holiday: A drug holiday is taking a two-day break from medication in order to lessen sexual side effects and plan intercourse during that period of time. The idea first emerged when patients informed their physicians that they had tried stopping their medication for a day or two and that this resulted in an improvement of sexual functioning without a worsening of depressive symptoms. Due to this finding, a study was performed to determine whether drug holidays were effective strategies for treating SSRI-induced sexual dysfunction. The patients taking sertraline and paroxetine reported improved sexual functioning, while the patients on fluoxetine did not. None of them experienced a worsening of their symptoms.10
- Pharmacological antidotes: Although not approved by the FDA for this particular use, numerous pharmacologic agents have been successfully used for treatment of sexual dysfunction caused by SSRIs. However, most of the information obtained regarding these antidotes has come from anecdotal case reports and not double-blind comparative studies, which means the data is significantly less reliable.
Some patients report that sexual dysfunction decreases over time, a phenomenon also known as spontaneous remission. However, this data is limited and it seems as though improvements occur when the initial complaints are mild and associated with delayed orgasm, rather than desire or arousal disorders.
Concluding Remarks
Schizophrenia can negatively impact sexuality by decreasing the quality of a person’s sexual relationships and also by schizophrenia-related medications’ inhibition of the sexual response cycle. Although uncommon, schizophrenia is a serious mental illness that should not be handled alone. Fortunately, schizophrenia can often be managed through medications and/or therapy and individuals affected by schizophrenia can go on to have healthy and happy lives. If you or a loved one are experiencing any symptoms of the depressive disorders mentioned in this article, contact your doctor or mental health care provider. Here are some resources: United States National Suicide Hotline: +1 (800) 273-8255 crisis call line 24 hours a day 7 days a week, or visit https://suicidepreventionlifeline.org/. United States National Institute of Mental Health Information Center: +1 (866) 615-6464 Monday through Friday, 8am-8pm (EST) or visit https://www.nimh.nih.gov/site-info/contact-nimh.shtml. References
- Schizophrenia Facts and Statistics. Schizophrenia.com: 2014.
- Boer, Marrit et al. The Facts About Sexual (Dys)function in Schizophrenia: An Overview of Clinically Relevant Findings. Schizophrenia Bulletin: 2015.
- Schizophrenia Overview. Mayo Clinic: 2016.
- A Family History Study of Schizophrenia-Related Personality Disorders. The American Journal of Psychiatry: 2006.
- Schizophrenia and Dangerous Behavior. LivingWithSchizophreniaUK.com: 2018.
- About Antipsychotic Drugs. PsychGuides.com: 2018.
- Park, Yeon et al. Antipsychotic-Induced Sexual Dysfunction and Its Management. The World Journal of Men’s Health: 2012.
- Medication. Anxiety and Depression Association of America: n.d.
- Major Depression with Psychotic Features. Medline Plus: 2016.
- Higgins, Agnes et al. Antidepressant-Associated Sexual Dysfunction: Impact, Effects, and Treatment. National Center for Biotechnology Information: 2010.
Last Updated: 8 February 2018.