A hysterectomy is a surgical procedure in which a female’s uterus is removed. In the United States, hysterectomies are very common, with 1 in 3 women undergoing the procedure by age 60.1 It is the second most common surgical procedure in reproductive-aged women.1 Hysterectomy rates vary in other countries, but the United States contains the highest rates.2 Hysterectomies are performed for various reasons, and there are different types of surgical methods that can be used. Sometimes, reproductive structures other than the uterus are removed. Because a hysterectomy removes the uterus, which carries a child to term, a female cannot have a biological pregnancy after the surgery. If a female wishes to have children afterwards, other options should be taken into consideration. As with all major surgeries, there are risks involved and recovery instructions are very important to follow.
Table of Contents
Reasons to Have a Hysterectomy
Certain health problems may lead a woman to consider having a hysterectomy. Since a hysterectomy is a major surgery, consult a doctor to learn about all possible treatment options before making the decision to have your uterus removed. A hysterectomy may be the best course of treatment if you have cancer of the uterus, cervix, ovary or endometrium.3 If this is the case, a doctor will be able to determine what type of cancer it is, what stage it is in, and whether additional treatments such a radiation and chemotherapy are needed.3 Besides cancer, a hysterectomy is a viable option for other health concerns:
- Uterine fibroids: Noncancerous growths within the uterine wall that may cause pain and bleeding.
- Heavy vaginal bleeding: Prolonged bleeding caused by hormone changes, fibroids, infection, or cancer.
- Uterine prolapse: The uterus slips from its place and falls into the vagina which can cause urinary or bowel problems and pelvic pressure. This is more common in women who have had multiple vaginal births.
- Endometriosis: A condition in which the tissue that normally lines the uterus grows on the outside of the uterus and ovaries. This can cause severe pain and bleeding.
- Adenomyosis: A condition in which the tissue that normally lines the uterus grows inside the walls of the uterus, which causes the walls of the uterus to thicken. This can also cause severe pain and bleeding.3
Consult a doctor to determine if a hysterectomy is the right treatment option for you if you have one of the above health problems.
Alternatives to a Hysterectomy
Each of the health problems mentioned previously have alternative treatment options that should be considered before opting for a major surgery. Some critics argue that many hysterectomies are performed unnecessarily. Additionally, some females decide to wait to have a hysterectomy until they are finished having children.4 “Watchful waiting” is an alternative approach that entails waiting and observing symptoms to see if they improve on their own.5 In the case of uterine fibroids, these growths tend to shrink after menopause, so a hysterectomy may not be necessary.3 The following alternative treatments further depend on the health condition:

- Exercise: Kegel exercises can help with uterine prolapse by restoring the muscles that hold the uterus in place.
- Medicine: Over-the-counter pain medications and hormonal birth control can help with heavy bleeding and pain associated with endometriosis.
- Vaginal pessary: A pessary is a plastic or rubber device that holds the uterus in place after a uterine prolapse.
- Uterine artery embolization (UAE): This procedure shrinks fibroids using plastic or gel particles which block the blood flow that supplies the fibroid. You cannot get pregnant after UAE.
- Surgery to treat endometriosis: A laparoscopic surgery removes scar tissue and growths without harming the surrounding organs.
- Surgery to stop heavy or long–term vaginal bleeding: Dilation and curettage (D&C) removes the uterine lining that builds up each month and can also remove noncancerous growths and polyps from the uterus. Endometrial ablation destroys the uterine lining permanently. You can still get pregnant after D&C, but you cannot get pregnant after endometrial ablation.
- Myomectomy: Myomectomy is a surgery that removes uterine fibroids without removing the uterus. It can be done through the pelvic area or the vagina and cervix. You can still get pregnant after a myomectomy.
- Myolysis: This surgery heats uterine fibroids, causing them to shrink and die, without removing the uterus. This surgery can be done laparoscopically. You can still get pregnant after myolysis.
- Magnetic resonance (MR)–guided focused ultrasound (MR[f]US): This procedure heats and shrinks fibroids with ultrasound waves. You cannot get pregnant after this procedure.3
All treatments should be discussed in-depth with a doctor before deciding if a hysterectomy is the right option. Depending on an individual’s situation, a hysterectomy may be the only option to relieve symptoms and provide much-needed relief.
The Specifics of a Hysterectomy
Once it has been decided that a hysterectomy is the best treatment option, other factors must be considered. There are different types of hysterectomies that remove different parts of the reproductive structure, as well as different methods to perform the surgery. Each of these variables is dependent on the reason for surgery and personal health history.
Types of Hysterectomies
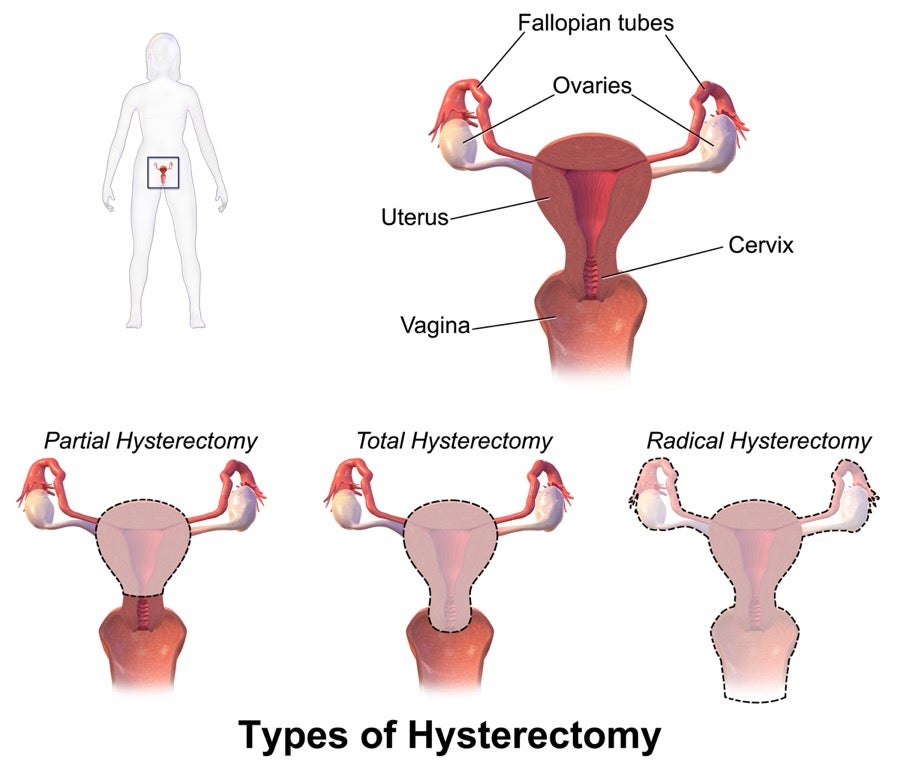
The most common type of hysterectomy is a total hysterectomy. This procedure removes all of the uterus and the cervix.3 However, there are other types of hysterectomies that may be performed depending on the condition that is being treated. A partial hysterectomy, also called a subtotal or supracervical hysterectomy, removes the upper part of the uterus but leaves the cervix intact.3 Lastly, a radical hysterectomy removes all of the uterus, cervix, tissue surrounding the cervix, and the upper part of the vagina.3
In all cases, the ovaries and fallopian tubes may be left or removed. Whether they are removed depends on the reason for surgery.3 In addition, a female may experience symptoms of menopause, depending on if the ovaries were removed during a hysterectomy.3 All females who undergo a hysterectomy will stop having their period, but if the ovaries are removed during the procedure, they will also have menopausal symptoms right away. Ovaries secrete the female sex hormones, estrogen and progesterone. Because hormone levels will drop quickly, menopause symptoms may be stronger than those caused by natural menopause.3 In procedures in which the ovaries are left intact, menopause symptoms will not appear right away, but they may begin a few years earlier than the average age for natural menopause (52 years).3 Removing the ovaries also eliminates the risk of ovarian cancer, but may increase the chance of heart disease due to estrogen’s role in heart health.5 Choosing to remove the ovaries during a hysterectomy should be carefully considered and discussed with a doctor.
How a Hysterectomy is Performed
A hysterectomy may be performed multiple ways. The method that is chosen will depend on the reason for the surgery:
- Abdominal hysterectomy: In an abdominal hysterectomy, incisions are made in the lower abdomen.3 Abdominal hysterectomies are associated with more complications, such as infection, bleeding, blood clots, and nerve and tissues damage.4
- Vaginal hysterectomy: A vaginal hysterectomy is performed through small cuts in the vagina.3 A vaginal hysterectomy is usually the first choice because there is a lower risk for complications during surgery and also a shorter healing time.4
- Laparoscopic hysterectomy: In a laparoscopic hysterectomy, the doctor makes small cuts to insert the laparoscope and tools into the body. The uterus is then removed through cuts made in the abdomen or vagina.3
- Robotic hysterectomy: The last method is a robotic hysterectomy. During this procedure, the doctor guides a robotic arm through small cuts made in the lower abdomen.3 Laparoscopic hysterectomies also present a lower risk for complications and pain but can take longer especially when done robotically.4
There are many factors that need to be considered when deciding which type of hysterectomy will be performed and how it will be done. A doctor will be able to determine which course of action is best. Sometimes, doctors wait until the surgery has begun to decide which method to use, allowing them to assess the internal conditions and proceed accordingly.4
Recovery
Recovery times vary depending on the method used to perform the hysterectomy. It is important to follow all directions given by the doctor for post-surgery recovery. Some females stay in the hospital for up to 2 days following surgery, whereas some females are sent home the day of the surgery.3 If cancer was the reason for surgery, hospital stays are usually longer.3 For an abdominal surgery, it takes between 4-6 weeks to recover, while a vaginal, laparoscopic, or robotic surgery takes between 3-4 weeks.3 Do not lift heavy objects for 4-6 weeks after surgery and make sure to get plenty of rest.3 While being mindful of limitations, getting up and moving around is beneficial for recovery as well.4 After surgery refrain from having sex or inserting anything into the vagina for 6 weeks after surgery, including tampons, and douches.4 After the recovery period, all normal activities can be resumed.
Life After a Hysterectomy
A hysterectomy is a major surgery that should only be performed if medically necessary. The most positive outcome from having a hysterectomy is relief of symptoms that made the surgery necessary in the first place. Other significant changes include no longer having a menstrual period and an inability to become biologically pregnant. Family planning is an important step in the life of a woman who may need a hysterectomy. Some women decide to wait to have a hysterectomy until they are done having children. If you wish to have a baby after surgery, assisted reproductive technology offers the ability to have a biological child. This is only possible if the ovaries were not taken out during surgery. A gestational carrier is an option for women who can produce healthy eggs but cannot carry a child to term. In this case, another woman is impregnated with an embryo that is the product of a couple or egg and/or sperm donor. Surrogates and adoption are also options for adding children to the family.

Menopause symptoms are also expected after having a hysterectomy. These symptoms include hot flashes, vaginal dryness, and cessation of menstrual periods. Hormone therapy may be advised if symptoms are severe, but this should be discussed with a doctor. Vaginal dryness may cause discomfort during sexual intercourse; using personal lubricants may make sexual intercourse more pleasurable after a hysterectomy. Increasing time spent on foreplay can also help sexual intercourse feel more comfortable by allowing the muscles in the vagina to relax and allowing more time for natural lubrication. If the ovaries are removed, the sudden drop in hormones may have an effect on libido. In addition, removal of the ovaries may increase one’s risk to other health conditions such as heart disease, osteoporosis, and urinary incontinence.3 Some females report an improved sex life after a hysterectomy because it relieves the pain associated with their previous health condition. Other women may experience a decrease in sensation. It’s important to communicate with your partner about what you are feeling both emotionally and physically to ensure that you are having an enjoyable experience.
Grief and depression may be felt after a hysterectomy due to the loss of fertility.3 Experiencing a range of emotions is normal after a major surgery such as this. If you are experiencing symptoms of depression that persist for a few weeks after the surgery, contact your doctor.
Concluding Remarks
A hysterectomy is a life changing surgery. When medically necessary, the relief of symptoms experienced afterwards is often more important than the inability to have a biological pregnancy. Women who wish to have children after a hysterectomy still have the ability to do so through assisted reproductive technology and adoption. Working closely with a doctor is important in considering all the options but in the end, the outcome could be life-saving.
References
- “Reproductive Health.” Centers for Disease Control and Prevention, Centers for Disease Control and Prevention, 17 Feb. 2017
- “Hysterectomy Statistics.” Hysterectomy Association
- “Hysterectomy.” Womenshealth.gov, 15 Oct. 2018
- “Women’s Health Care Physicians.” Group B Strep and Pregnancy – ACOG
- “Hysterectomy.” NWHN, 28 Nov. 2016
Last updated: 20 January 2019